Have Smokers Been Hoodwinked
and Bamboozled by Placebos?
Has the greatest medical research sham in history been perpetrated upon smokers? Have tens of millions purchased and used expensive quitting products that were actually less effective than quitting without them? If so, how could this happen?
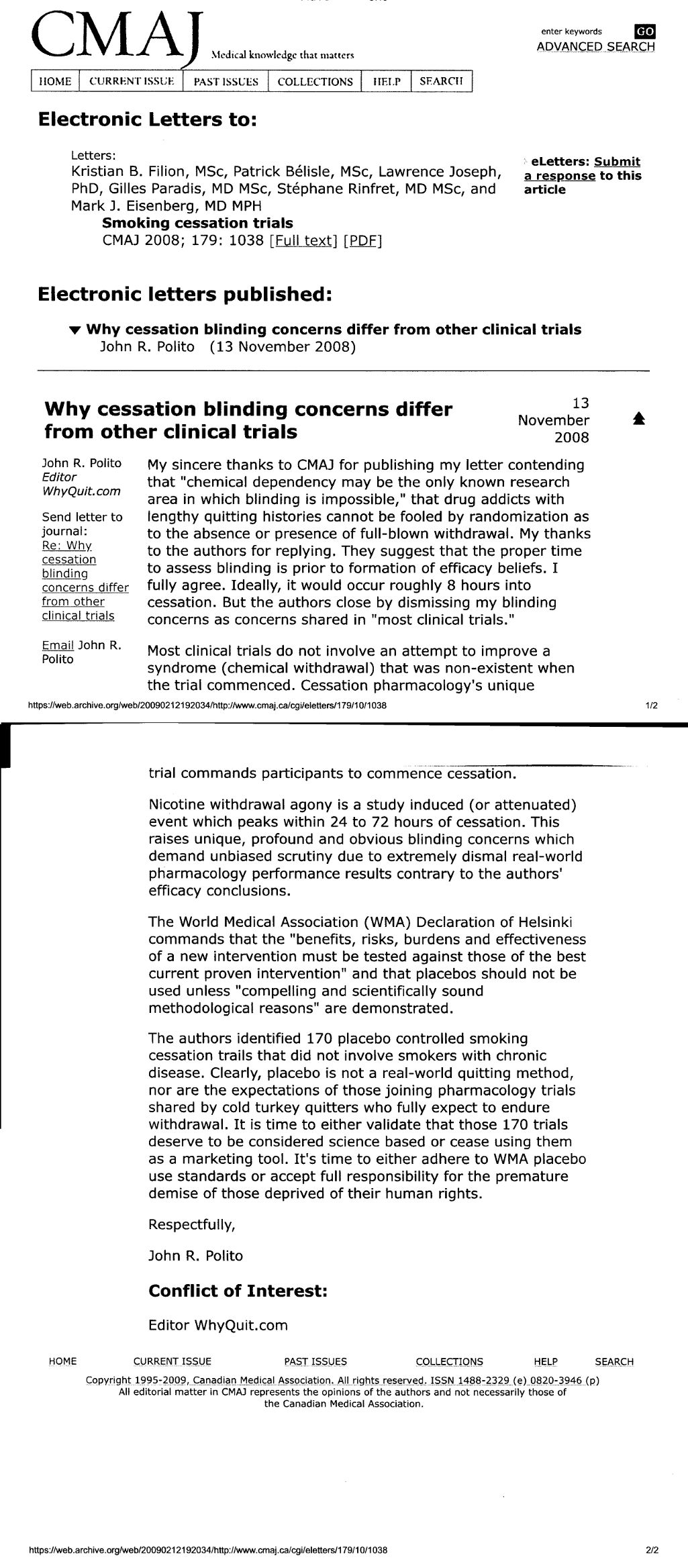
Canada's leading medical journal is hosting a debate as to whether or not participants in nearly 200 placebo-controlled quit smoking studies could tell if they had been randomly assigned to use an inert placebo device or a real replacement nicotine delivery device (an NRT product) such as the gum, lozenge or patch.
The current issue of the Canadian Medical Association Journal (CMAJ) shares a letter submitted by this writer (John R. Polito), which contends that the onset or absence of physical withdrawal destroys blinding, that "pharmacologic treatment of chemical dependency may be the only known research area in which blinding is impossible."
Cessation pharmacology experts responded to the letter by asserting that "blinding is undoubtedly a key component of the validity of inferences drawn from randomized controlled trials" and that "maintaining blinding may be difficult, particularly if study participants experience withdrawal symptoms."
The experts closed by asserting that "incomplete blinding is a potential limitation to most clinical trials." I responded pointing out how smoking cessation clincal trials differ from "most clinical trials."
If successful study blinding is key to the scientific validity of 26 years of pharmacology study findings then why is no expert willing to assert that NRT, Zyban or Chantix studies have been blind? Frankly, they can't. The only study to review clinical trials that assessed blinding was published in 2004. It found that "subjects accurately judged treatment assignment at a rate significantly above chance."

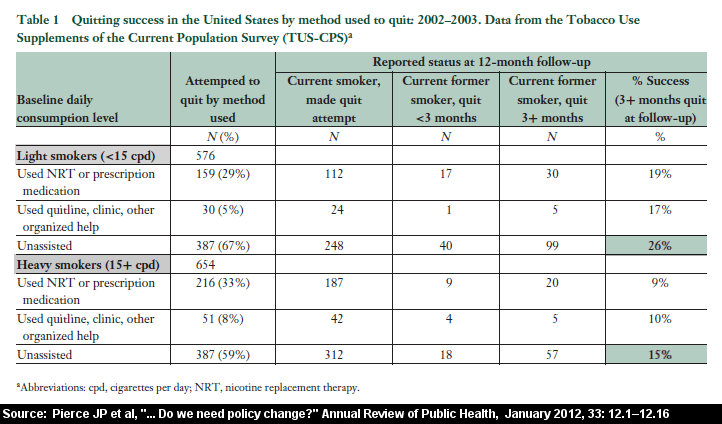
Pharmaceutical quitting products easily and routinely defeat placebo users inside clinical trials, yet fall flat on their face when going head-to-head against cold turkey quitters in real-world use (see the 2018 Weaver study, this July 2013 Gallup Poll; this chart from Pierce JP, 2012, also see 2006 Unpublished U.S. National Cancer Institute Survey of 8,200 quitters, as reported in the Wall Street Journal, Page A1, February 8, 2007; also see Doran CM, et al, Smoking status of Australian general practice patients and their attempts to quit [PubMed Abstract], Addict Behav., 2006 May;31(5):758-66; also see, Ferguson J, The English smoking treatment services: one-year outcomes, Addiction [PubMed abstract], 2005 Apr;100 Suppl 2:59-69 [see Table 6]; also see, Alberg AJ, et al, Nicotine replacement therapy use among a cohort of smokers [PubMed abstract], J Addict Dis., 2005;24(1):101-13; also see, SmokeFree London, Tobacco In London, Facts and Issues, [online PDF report, see Figure 14], November 26, 2003; also see Boyle RG, et al, Does insurance coverage for drug therapy affect smoking cessation? [free full-text], Health Aff (Millwood), 2002 Nov-Dec;21(6):162-8; also see, Pierce JP, et al, Impact of Over-the-Counter Sales on Effectiveness of Pharmaceutical Aids for Smoking Cessation [free full text], JAMA, September 11, 2002;288:1260-1264).
Clearly, placebo is not a real quitting method, and cold turkey quitters normally do not join clinical studies seeking medications that promise to lessen their withdrawal syndrome. Their objective is to endure withdrawal and move beyond it.
While the pharmacology quitting product era promised to double quitting rates it has instead brought decline in the U.S. smoking rate to a standstill. How many thousands of smokers repeatedly believed the "double your chances" slogan, repeatedly relied on it in using "medicines," and died trying? How many believed that the quitting aid they purchased had been scientifically proven to be the best option available?
The question at the center of the debate is really rather simple. Can a nicotine addict who is badly in need of nicotine fix tell whether or not nicotine replenishment has occurred? If so, and they can do so within a few hours of quitting, have researchers been honest in labeling their studies blind and declaring them "science-based?"
Principle 32 of the World Medical Association's (WMA) Declaration of Helsinki commands that the "benefits, risks, burdens and effectiveness of a new intervention must be tested against those of the best current proven intervention" and that placebos should not be used unless "compelling and scientifically sound methodological reasons" are demonstrated.
The pharmaceutical industry and FDA contend that nicotine gum was proven effective prior to 1984. If true, why the need for 200 placebo controlled trials since 1984? Is it because placebo is easiest to beat, or that stockholders are more important than the lives of the tens of thousands smokers assigned to placebos since 1984?
If researchers refuse to honor the smoker's human rights, do they assume responsibility for the demise of relapsing placebo users left so demoralized that there wasn't sufficient time, prior to being claimed by their addiction, to muster the confidence to try a truly effective method?
The problem is that U.S. cessation research is an utter mess, that locating a clincal trial involving "real" cold turkey quitters is nearly impossible. Any researcher whose research findings damage pharmaceutical industry financial interests can probably forget industry study funding for the rest of their life.
We need common sense laws and ethics that protect the independence and integrity of clincal trial researchers. We need greater government funding of research that's medically indicated, not just research with potential to handsomely reward corporate shareholders. Our nation's leading cause of premature demise, the time is now for serious and immediate independent research into whether or not 200 placebo controlled quit smoking studies reflect true science or history's greatest study sham ever.
Canadian Medical Association Journal References
John R. Polito is solely responsible for the content of this article. Any factual error will be immediately corrected upon receipt of credible authority in support of the writer's contention. E-mail comments to john@whyquit.com
{kind=link}
{kind=link}
