90% of Ex-smokers Quit Smoking Cold Turkey
 In that New Year's is by far the biggest quitting time of the year, smokers are being bombarded with ads attempting to convince them to betray their natural instincts. What pharmaceutical companies dare not reveal is that during 2006 almost all long-term successful quitters again succeeded by ending all nicotine use, not by replacing it by use of the nicotine gum, nicotine patch or new "cherry flavored" nicotine lozenge (NRT or Nicotine Replacement Therapy), or by using designer
drugs that attempt to imitate it (Chantix or Zyban).
In that New Year's is by far the biggest quitting time of the year, smokers are being bombarded with ads attempting to convince them to betray their natural instincts. What pharmaceutical companies dare not reveal is that during 2006 almost all long-term successful quitters again succeeded by ending all nicotine use, not by replacing it by use of the nicotine gum, nicotine patch or new "cherry flavored" nicotine lozenge (NRT or Nicotine Replacement Therapy), or by using designer
drugs that attempt to imitate it (Chantix or Zyban).
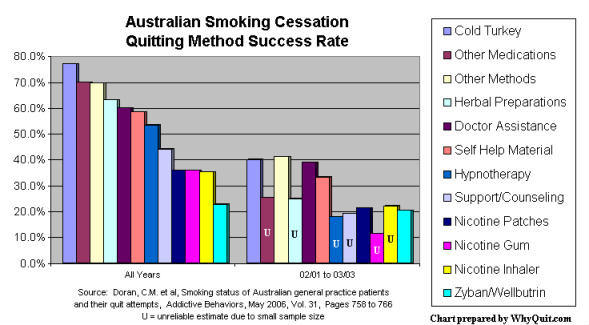
Relying upon survey data, in 1992 the U.S. Centers for Disease Control (CDC) reported that "approximately 90% of successful quitters have used a self-help quitting strategy, most by quitting abruptly." Looking back at survey data, in 2000 the Surgeon General reported that, "historically, the great majority of smokers (more than 90 percent) who successfully quit smoking did so 'on their own'" (see PDF page 6). In 2006, an Australian study following smoking patients of family practice physicians found that cold turkey quitters accounted for 1,942 of 2,207 former smokers, a whopping 88% of all success stories.
Even more disturbing, the Australian study, published in the May 2006 edition of Addictive Behaviors, found that the success rate for cold turkey quitters was twice as high as the rates for those using the nicotine patch, nicotine gum, nicotine inhaler or Zyban (bupropion).
After more than two decades of wide-spread NRT use the pharmaceutical industry cannot point to a single real-world performance evaluation in which those quitting with NRT performed better than those quitting without it. None.
A September 2002 Journal of the American Medical Association study concluded that "NRT appears no longer effective in increasing long-term successful cessation in California smokers." The California finding is backed by quitting surveys from Minnesota, Quebec, London and Western Maryland.
It is also backed by a study published in the April 2005 edition of Addiction that surveyed quitting rates from England's National Health Service quit smoking program. There, 25.5% of cold turkey quitters were still not smoking at one year, compared to only 15.2% of NRT quitters, 14.4% of Zyban users, and 7.4% of those using both NRT and Zyban at the same time.
How can this possibly be correct? Unlike the U.S., the cost of using NRT and Zyban is government subsidized in England and Australia, making them available to all. For years we've heard pharmaceutical company marketing claim that these products double your chances. Who is telling the truth? What's going on?
The answer rests in the difference between "efficacy" and "effectiveness." When pressed, most marketing NRT, Zyban and Chantix will openly admit that their marketing assertions are based upon clinical efficacy findings not effectiveness.
"Efficacy" findings are a product of highly manipulated randomized double-blind clinical trials conducted under what researchers hope are ideal conditions. They are big on internal controls but at the expense of being unable to generalize findings as applying to quitting populations not studied or quitters quitting under different conditions.
"Effectiveness" evaluations, on the other hand, evaluate how quitting methods perform in real-world populations under real-world conditions. While high in external validity they lack controls. Effectiveness evaluations can be quick, simple and inexpensive. When you ask 1,000 former smokers if they tried quitting last year, and if so what method they used and whether or not they succeeded, it's a little hard to make a mistake or manipulate outcome. What you see is what you get.
Although clinical trial researchers and pharmaceutical influence have condemned quitting method surveys as "unscientific" the scientific integrity of their own work has now been completely undermined. A June 2004 study found that NRT clinical trials were generally not blind as claimed in that "subjects accurately judged treatment assignment at a rate significantly above chance."
If clinical trial participants could tell whether or not their nicotine gum or lozenge was delivering nicotine or was instead an empty placebo, it could explain why NRT efficacy is so high in clinical trials yet falls flat on its face the moment it exits the trial clinic's doors.
Are NRT, Zyban and Chantix clinical study results grounded in science or do they instead reflect fulfilled or frustrated expectations associated with a quitter either sensing or not sensing some degree of reduction in their own personal withdrawal syndrome, a syndrome that those with any prior quitting history might find difficult to forget?
Imagine the cornerstone of an entire nation's quitting policy resting upon studies that were not blind, upon efficacy conclusions reflecting junk or pseudo science. Is it possible that scores of cessation pharmacology "experts" have built research careers and academic reputations upon the biggest sham ever perpetrated upon smokers?
If cessation pharmacology eventually proves to have been a complete sham upon smokers it does not follow that all involved were charlatans, or necessarily motivated by financial conflicts of interest, or knew it was a sham. I'm convinced that most are good, decent and well intentioned folks who were caught up in "group think." Their greatest fault was in accepting rather than challenging what to them seemed like well-established foundations.
 What it would mean is that researchers were horribly wrong in convincing
millions upon millions to believe their conclusions about over-the-counter NRT
products, products we now know produce a 93% failure rate and nearly a 100% failure rate among those making a second try.
What it would mean is that researchers were horribly wrong in convincing
millions upon millions to believe their conclusions about over-the-counter NRT
products, products we now know produce a 93% failure rate and nearly a 100% failure rate among those making a second try.
It would be refreshing if during 2007 health agencies and researchers at last started being open and honest with smokers about how almost all long-term successful quitters quit during 2006. Smokers are entitled to the truth. They can handle it. It would also be great to hear them admit that, out here in the real-world, cold turkey has yet to be defeated in any head-to-head competition to date.
In October the CDC reported that for the first time since 1997 the U.S. smoking rate failed to decline. In June 2000, U.S. cessation policy not only turned its back on cold turkey quitters, quitting lessons shared by the CDC and all other government agencies started interfering with natural school of hard-quitting-knocks lessons. Through repeated attempts most smokers were eventually able to discover that putting any nicotine back into their bloodstream, even one puff, meant that they had to go back to square one and start all over again.
Instead of teaching the "Law of Addiction" and the need to end all nicotine use the CDC muddies the mind and confuses all prior relapse lessons by teaching every smoker and quitter visiting its website that nicotine is "medicine" and "key to quitting" is to "get medication and use it correctly."
If granted one wish during 2007 it would be for the U.S. government to immediately repeal U.S. Cessation Guideline Recommendation 7 which currently reads, "Numerous effective pharmacotherapies for smoking cessation now exist. Except in the presence of contraindications, these should be used with all patients attempting tobacco cessation." Not with "some" patients but "all."
Repeal would be based upon one simple premise. After 22 years, cessation pharmacology cannot produce a single shred of real-world proof of effectiveness in going head-to-head with those quitting without it. To watch government teach smokers that nicotine cessation is wrong, that instead they need to replace it, is an insane policy that's costing lives.

{kind=link}
